
Variables used for computing the propensity score of ATG use.

Hazard ratio for OKT3 vs ATG useage and 95 % confidence intervals are nearly the same, when missing data are replaced by the median of the respective group.
Red lines represent the models computed with data missing, black lines represent the hazard ratio and 95 % confidence interval when missing data are replaced.
Modification of hazard ratio for OKT3 vs. ATG usage in the automated model, which is calculated as a bivariable model

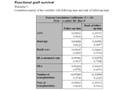
Correlation matrix of the Schoenfeld residuals of variables used in the model for functional graft survival with followup time and rank of followup time

Schoenfeld residuals for functional graft survival.

Correlation matrix of the Schoenfeld residuals of variables used in the model for actual graft survival with followup time and rank of followup time

Schoenfeld residuals for actual graft survival.
Correlation matrix of the Schoenfeld residuals of variables used in the model for patient survival with followup time and rank of followup time

Schoenfeld residuals for patient survival.

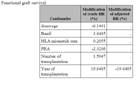
Analyses with first transplantation only.
Associations between OKT3 use and functional graft loss using different model-building strategies
Analyses with first transplantation only.
Associations between OKT3 use and actual graft loss using different model-building strategies

Analyses with first transplantation only.
Forest plot of hazard ratios for OKT3 use.
Analyses with first transplantation only.
Associations between OKT3 use and patient mortality using different model-building strategies
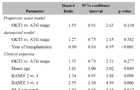
Analyses with patientes who experienced BCAR in the first three months of the first transplantation.
Associations between OKT3 use and functional graft loss using different model-building strategies
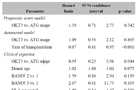
Analyses with patientes who experienced BCAR in the first three months of the first transplantation.
Associations between OKT3 use and actual graft loss using different model-building strategies
Analyses with patientes who experienced BCAR in the first three months of the first transplantation.
Forest plot of hazard ratios for OKT3 use.
Analyses with patientes who experienced BCAR in the first three months of the first transplantation.
Associations between OKT3 use and patient mortality using different model-building strategies